A Minimally Invasive Implant for Diagnosis and Treatment in Refractory Epilepsy
Clinical Needs
Epilepsy affects 60 million people worldwide, and is characterized by seizures ranging from a temporary loss of awareness to total loss of consciousness. Epilepsy etiology is often multifactorial. People with epilepsy have a higher risk of personal injury, are three times more likely of premature death, and are at risk of sudden unexpected death in epilepsy (SUDEP). The impact of epilepsy also extends to unemployment, underemployment, depression, and anxiety, which significantly influences life quality of patients.
Seizures occur unpredictably. Even in those whose seizures are controlled on medications, breakthrough seizures can occur on and after weaning off medication. For those whose seizures are not controlled, the frequency can be anything from days, to weeks, or months. Seizures commonly happen at night, when caregivers are not aware. In the hospital setting seizures may be missed, particularly in those with subtle clinical signs. In the intensive care setting, non-convulsive status epilepticus (prolonged seizures on EEG without visible physical movements) can go undetected in patients with neurological insults. In patients with frequent seizures, sustained monitoring would aid seizure detection to accurately determine seizure frequency and provide a platform on which to build other modalities such as seizure localization and responsive neurostimulation.
Novel technologies to facilitate long-term monitoring at the bedside and at home are required to provide better diagnosis and treatment.
- Low-power, miniaturized hardware system would reduce the labour load for clinical routine EEG recordings and ease long-term EEG recordings, extending their applicability beyond the hospital setting into the community and home. Implanted hardware system has the potential to form a link in implantable seizure detection and control systems and rehabilitation/brain controlled prostheses.
- Novel solutions to remove artifacts from EEG and permit clearer interpretation of EEG ictal patterns are required for a better diagnosis in epilepsy.
- The combination of miniaturized EEG hardware, artifact removal and seizure detection would facilitate the widespread use of automated EEG systems to detect seizures in both hospital and home settings. Expert systems can enhance medical and home care.
Research Overview
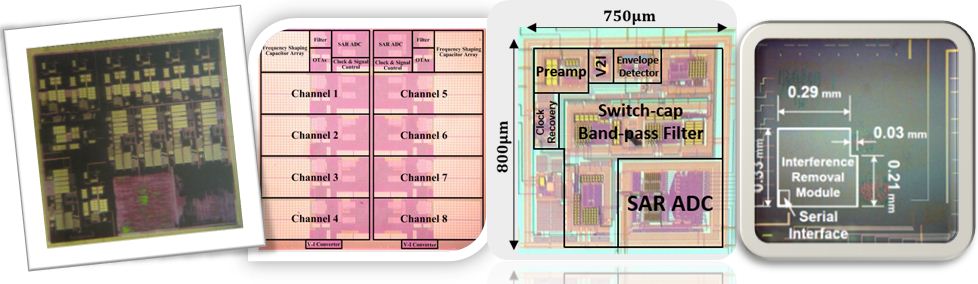
The proposed design has two microsystems: one implant microchip buried under the skin and one wearable earpiece. The implant chip is suitable for recording both regular EEG data (0.1-100Hz) and high-frequency oscillations (up to 800Hz). It consists of a low noise amplifier, chopper spike filter, variable gain buffer, configurable-bit-bandwidth delta-sigma modulator, decimation filter, and embedded memory for data acquisition and processing. When measured at 35µA/1.2V supply, the recorder noise is 0.46µV for 0.1-100Hz and 0.98µV for 0.1-800Hz, and the recording precision is 15-bit.
The second microsystem is inside the earpiece, which includes a power amplifier to wirelessly power up the implant, a data receiver to collect EEG data, and a signal processor. So far we have the power and data telemetry units developed. The power link works at a 10MHz carrier frequency and can deliver 1-10mW to the implant. The data demodulator can recover data from a weakly modulated power carrier (below 1% modulation index), where the measured data rate can go beyond 1Mbits-per-second. The proposed power and data links can penetrate through the skin and are able to support 32-channel high frequency EEG data acquisition. We also have a customized wireless transceiver board (about 1 by 2 cm) that can relay the data from the earpiece to a remote station for patient data storage. The communication distance is over 10 meters.
Experiments on humans and monkeys are in preparation. For human experiments, they are prolonged scalp EEG recordings with epilepsy patients. For monkey experiments, they are sub-scalp EEG recordings with electrodes implanted for 6 months.
Sub-Scalp Implant Project Chip Gallery by TSS Group
Sub-scalp EEG Implant Microelectronics
We have proposed two types of recorders. The Type I neural recorder has an elegant feedback loop that features high precision data acquisition (less than 1µV noise, more than 15-bit dynamic range). This implementation will be suitable for seizure detection based on individual channels and is specially designed to accommodate motion/muscle artifacts. The Type II neural recorder is based on a novel architecture, which allows extremely low power operation (less than 2.5µW when sampled at 2.5kHz) that leads to small thermal stress on surrounding tissues and high input impedance (50Gohm at 1Hz) to dominate electrode encapsulation due to the response from the body immune system. It features small distortion, long-term reliability, and artifact suppression at the cost of an increased noise level (1.1µV at 0.1-100Hz or 1.3µV at 0.1-500Hz).
Type I Recorder
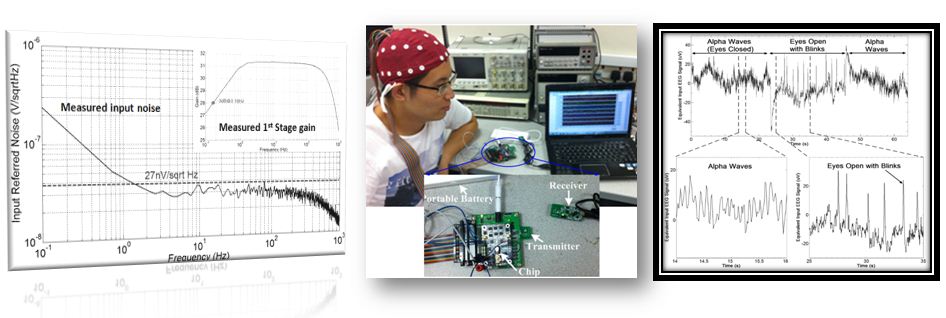
We have designed, fabricated, and tested a Type I recorder in the past one year. It consists of a configurable-DR low noise instrumentation amplifier, chopping spike filter, low pass filter, discrete-time variable gain switched-amplifier, and configurable-bit-bandwidth Delta-Sigma ADC. The amount of noise is 0.46µV when integrating to 100Hz (EEG data) and 0.98µV when integrating to 800Hz (high frequency oscillations). The Delta-Sigma ADC has a 101-dB peak-SNDR and a 102fJ/conv.-step FOM. The total current consumption per channel is 16µA measured at 100Hz/93dB or 35µA measured at 800Hz/93dB.
Type II Recorder
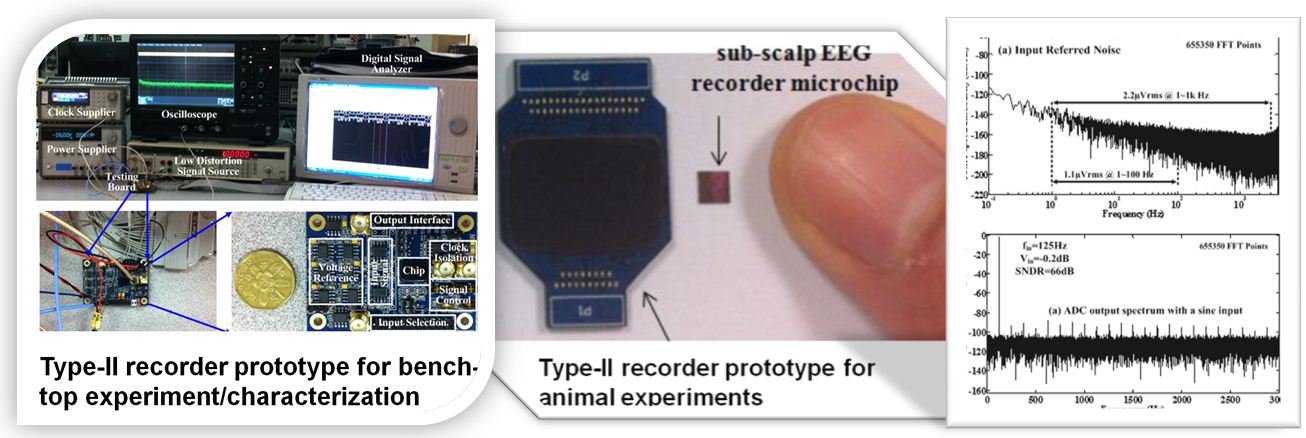
We have designed, fabricated, and tested a type II recorder, which consists of a modified frequency shaping amplifier, variable gain buffer, filter, and a 12-bit SAR ADC (66dB SNDR). Due to frequency shaping, the actual dynamic range of the recorder is several bits extended and is data dependent (>80dB in experiments). The measured noise is 1.1µV when integrating to 100Hz and 1.3µV when integrating to 500Hz. The total power consumption per channel is 2.5µW and the noise efficiency factor (NEF) of the frontend stage amplifier is 2.2. Compared with the Type-I recorder, the Type-II recorder consumes 10 times less power however with more noise.
Wireless Power and Data Link
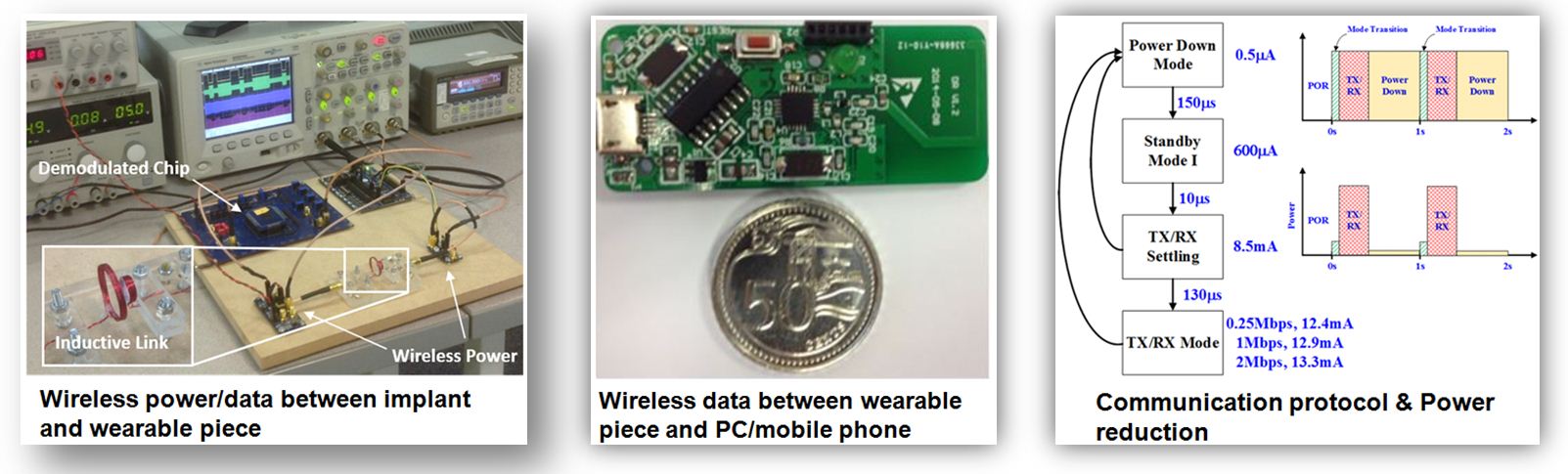
So far we have a wireless prototype that can deliver 1-10mW power to the sub-scalp implant at about 20% power efficiency (defined as the harvested DC power divided by the total power drained from battery). The implant coil is around 9mm in diameter (700nH) and the carrier frequency is set at 10MHz. Along with power transmission, it allows delivering data at 1Mbps through load-shift-keying (LSK) modulation from the implant to the earpiece. To increase the data rate and reduce disturbance to power transmission, a highly sensitive LSK demodulator chip has been designed. The demodulator consists of a multi-phase envelope detector that extracts and digitizes the envelope of the power carrier. We have designed a transceiver board using commercial chip, antenna, and USB interface, where the working distance is around 20 meters. This board relays sub-scalp EEG from the earpiece to a laptop for data storage and further signal processing. With a 400mAh external battery in the earpiece (10g, 150Wh/Kg, 3.6V), it can support continuous data acquisition from the implant to a laptop for one day.
Artifact Characterization, Detection, and Removal
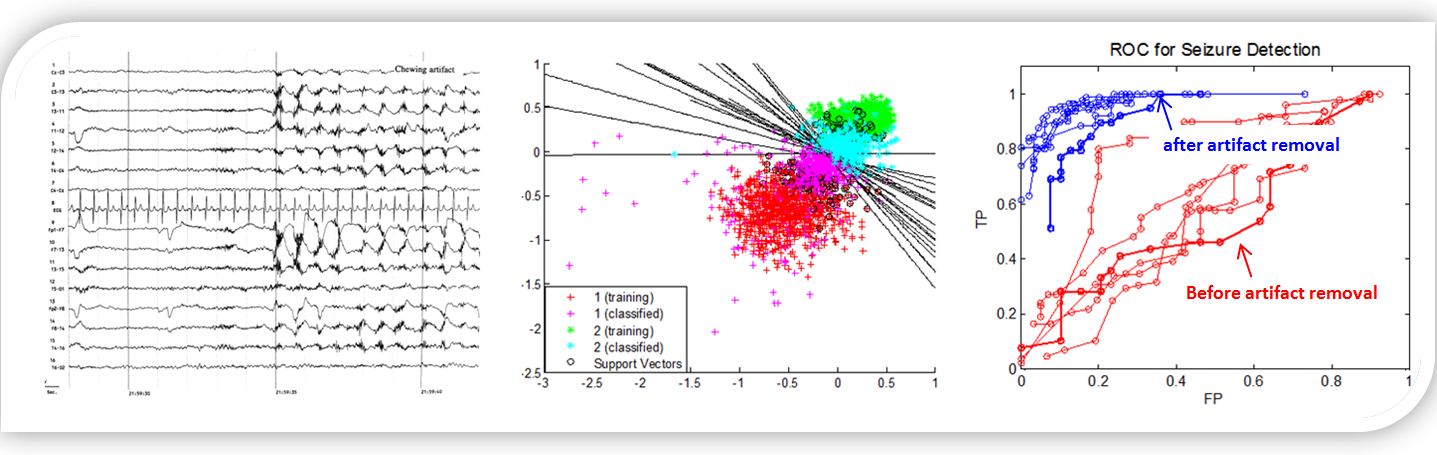
Artifacts are inherent in EEG recordings due to the low amplitude of brain electrical signals and the presence of non-cerebral electrical signals. This is particularly a problem in long-term monitoring, where seizures are captured and the onset may be obscured by muscle artifacts, and ambulatory monitoring, where patients may wear the electrodes at home and during their daily activities. We have tried to characterize artifacts present in an ambulatory environment followed by developing an automated algorithm that can remove artifacts as much as possible. We have compared the seizure classification/detection accuracy before and after artifact removal to observe if there is any significant improvement made. Our preliminary results suggest that the proposed artifact detection/removal algorithms can substantially improve a seizure detection ROC curve. The following artifacts have been included into our model: horizontal eye movement artifact, blink artifact, eye flutter artifact, electrode tapping artifact, jaw-clenching artifact, chewing artifact, dry electrode artifact, forehead rubbing artifact, and pulse artifact.
Power Line Interference Removal
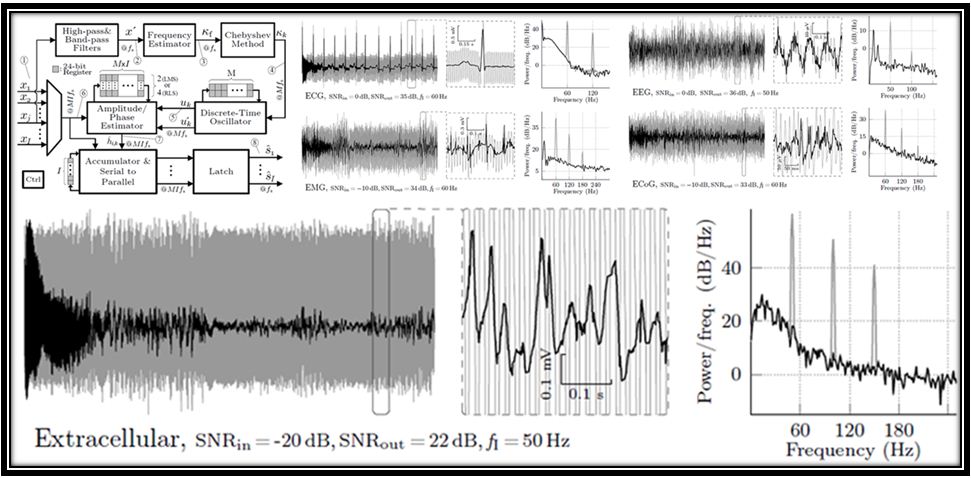
Power line interference may severely corrupt neural recordings at 50/60 Hz and harmonic frequencies. The interference is usually non-stationary and can vary in frequency, amplitude and phase. To retrieve the gamma-band oscillations at the contaminated frequencies, it is desired to remove the interference without compromising the actual neural signals at the interference frequency bands. In this work, we present a robust and computationally efficient algorithm for removing power line interference from neural recordings. The algorithm does not require any reference signal, and can track the frequency, phase and amplitude of each harmonic. When benchmarked with other popular approaches, our algorithm performs better in terms of noise immunity, convergence speed and output signal-to-noise ratio (SNR). While minimally affecting the signal bands of interest, the algorithm consistently yields fast convergence ( <100 ms) and substantial interference rejection (output SNR>30 dB) in different conditions of interference strengths (input SNR from -30 to 30 dB), power line frequencies (45-65 Hz), and phase and amplitude drifts. A hardware prototype was fabricated in a 65 nm CMOS process and tested. Software implementation of the algorithm has been made available for open access at https://github.com/mrezak/removePLI.